
+38(066)493-43-78
Показать все контакты

GUNA COLLAGEN MEDICAL DEVICES 10 YEARS ON − A REASONED ANALYSIS OF 2 RECENT IMPORTANT STUDIES AND LITERATURE UPDATE
Prof. Leonello Milani, MD, PhD – Scientific director of “La Medicina Biologica” and “Physiological Regulating Medicine” Via Palmanova, 71 I – 20132 Milano
THE INTELLIGENT TRIPLE HELIX
Collagen (COL) is the most common structural protein biopolymer in the connective tissues of animals; in humans, it represents 25-30% of all proteins (Schmidt & Burkhardt, 2001) and 6% of total mass (Wu, 2011).
– This fibrous protein, which gives the macroscopic and microscopic anatomical structures high mechanical resilience (traction), incompressibility and tensile strength, is prevalent in the skin and subcutaneous tissues, tendons, joint capsules, ligaments, cartilage and bone. In striated muscle, COL constitutes the main component of the endomysium (Light & Champion, 1984), the layer of areolar connective tissue that sheathes each individual muscle fibre, composed primarily by types I and II COL (Fratzl, 2008; Saladin, 2012).
– The function of COL, in addition to structuring, supporting and stabilising the somatic scaffold, is, unexpectedly, antioxidant, as demonstrated in vitro; adding COL to culture cells increases the activity of antioxidant enzymes such as superoxide dismutase (SOD), catalase (CAT) and phospholipid hydroperoxide glutathione peroxidase (GSH-Px) (Song et al., 2017), thereby preventing cell membrane damage caused by the ROS – reactive oxygen species (Alemán et al., 2011; Nakchum et al., 2016).
Type I COL alone accounts for ≈ 90% of all COL in vertebrates; so far, 29 types of COL have been identified (Söderhäll et al., 2007), according to their different composition, produced by fibroblasts; mesenchymal, epithelial and endothelial cells; chondroblasts; osteoblasts and odontoblasts (Hand & Ten Cate, 2006; Gartner & Hiatt, 2007; Shoulders & Raines, 2009).
– The synthesis of mature COL involves 7 intra- and extracellular steps, from pre-procollagen (2 steps) to procollagen (3 steps) to tropocollagen (1 step) to collagen (1 step).
.png) This complex and highly structured chain of events, which has been perfected over millions of years of evolution, can be interrupted or altered, causing, in humans, serious genetic diseases such as Ehlers-Danlos syndrome (abnormal positioning and spacing of the COL fibrils), Marfan syndrome (abnormal fibrillin 1 production), Alport syndrome (types I and IV COL synthesis defect), Osteogenesis imperfecta (type I COL synthesis defect); autoimmune diseases, such as SLE and systemic scleroderma and acquired diseases such as scurvy: many sailors of the past, in their voyages acrossthe oceans, have paid with their life a dietary deficiency of vitamin C (L-ascorbic acid), which is absolutely necessary for the synthesis – via proline – of hydroxyproline and – via lysine – of hydroxylysine: their tropocollagen was unable to come together in fibrils.
This complex and highly structured chain of events, which has been perfected over millions of years of evolution, can be interrupted or altered, causing, in humans, serious genetic diseases such as Ehlers-Danlos syndrome (abnormal positioning and spacing of the COL fibrils), Marfan syndrome (abnormal fibrillin 1 production), Alport syndrome (types I and IV COL synthesis defect), Osteogenesis imperfecta (type I COL synthesis defect); autoimmune diseases, such as SLE and systemic scleroderma and acquired diseases such as scurvy: many sailors of the past, in their voyages acrossthe oceans, have paid with their life a dietary deficiency of vitamin C (L-ascorbic acid), which is absolutely necessary for the synthesis – via proline – of hydroxyproline and – via lysine – of hydroxylysine: their tropocollagen was unable to come together in fibrils.
– Like all other ancient primitive molecules, COL bears witness to the fatal causal chain.
Its right-handed triple helix form (the individual non-coaxial left-handed helical chains come together, interweaving with one another, due to weak chemical bonds) (Ramachandran, 1955 in Bhattacharjee, 2005), its constitutional simplicity (repeated triplets of just 5 amino acids positioned in different ways), its biochemical immutability (the structure of COL is practically identical in all species, from invertebrates to man) and its structural and functional intelligence are guarantors of flawless function. In addition to composing tendons, bone, etc., COL enters by phylogenetic right also into the composition of the extra- and intra-cellular matrix and cytoskeleton (Tomasek et al., 1982; Qin et al., 2018).
– Nature loves schemes and modules, and repeats them as often as it can and whenever they are necessary.
Synthetic glucocorticoids, especially when fluorinated, despite guaranteeing high anti-inflammatory activity, slow down the synthesis of COL in vivo and in cell cultures (Cutroneo et al., 1981).
– Paradoxically, the class of drugs most commonly prescribed in Collagenopathies actually weakens the neosynthesis of COL, impairing its efficacy over time, thereby creating a vicious therapeutic loop that becomes increasingly difficult to overcome successfully.
.png)
• In humans, COL biosynthesis peaks between 40 and 60 years of age (collagen plateau) (in Heine, 2009) (FIG. 1); it diminishes rapidly in the sixth decade of life, together with the synthesis of elastin and the matrix proteoglycans (the total collagen pool is halved between 60 and 80 years of age).
.png) – This reduction is governed by the late-expression age-dependent genes that encode for collagenase [matrix metalloproteinases (peptidase) = MMPs (previously known as matrixine)] that prevail over the TIMPs (tissue inhibitors of metalloproteinases), MMP-inhibiting glycoproteins (Brew et al., 2000) (FIG. 2).
– This reduction is governed by the late-expression age-dependent genes that encode for collagenase [matrix metalloproteinases (peptidase) = MMPs (previously known as matrixine)] that prevail over the TIMPs (tissue inhibitors of metalloproteinases), MMP-inhibiting glycoproteins (Brew et al., 2000) (FIG. 2).
TheTIMPs, natural inhibitors of the MMPs and of the disintegrin metalloproteinase (Brew & Nagase, 2010), have an antiapoptotic function and are encoded by allocated genes on the X chromosome.
– This likely partly explains the greater longevity of female (XX allosomes) vs males (Aviv et al., 2005).
ACTH (Reichenstein et al., 2004), IL-10 (Lacraz et al., 1995), and IL-6 (Lotz & Guerne, 1991) stimulate TIMP-1, through the inhibition of the MMPs.
• It is important to remember that IL-6 plays a dual pro-inflammatory and anti-inflammatory role depending on the physiological or pathological context and the tissue it acts in. – IL-6 modulates the destruction of COL by the MMPs; its increase in the acute phase of inflammation prevents it from spreading within the affected tissue, restricting it by the hold/staying power of the local COL.
In COL remodelling, the discrepancy by which the degradation phenomena are not adequately compensated by synthesis leads, after ≈ 60 years of age, to a considerable loss of the structures primarily composed of COL with a consequent anatomical and functional weakening (in particular, chronoageing and musculoskeletal disorders
The protein chains that constitute COL are massive and difficult to “create” in a laboratory: so far, it has not been possible to produce them synthetically because of their post-translational modifications (Tanrikulu et al., 2016), due to problems of symmetry (Schmitt et al., 2009) and stability (Fields, 2010). COL for therapeutic use must necessarily be extracted from animal tissues.
GUNA COLLAGEN MEDICAL DEVICES
Since the presentation and introduction into peri- and intraarticular and soft tissue injection therapy of Guna Collagen Medical Devices (MDs) (Milani, 2010) various researchers have conducted on the therapeutic action of these products in the different medical conditions for which they were developed, many of which on the osteo-artro-myofascial system, 28 good-quality clinical trials, some of which were published in peer-reviewed, indexed international journals with high impact factors (BMC Musculoskeletal Disorders, Pain Research and Management, Current Medicinal Chemistry) (TAB. 1).
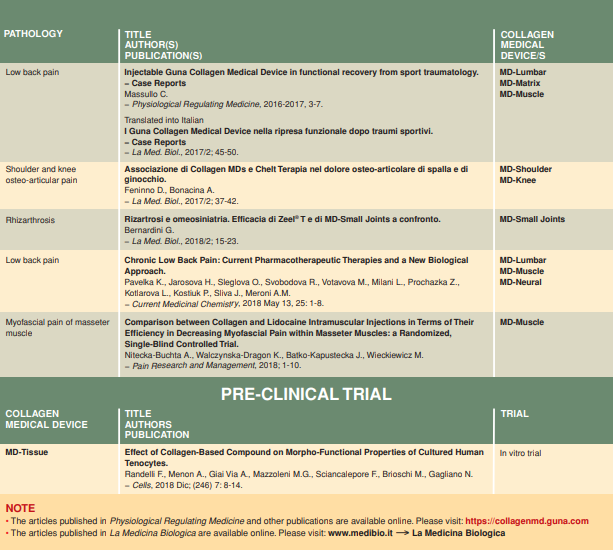
– In over half of these publications (16 out of 28) (TAB. 1), the authors consider a treatment combination of 2 or more medical devices (e.g. for chronic lower back pain: Pavelka et al., 2012, 2018).

