
+38(066)493-43-78
Показать все контакты

• The salient characteristics and a reasoned analysis of two important recent studies are provided below; the first is a clinical study, the second a basic (preclinical) study on the therapeutic and biological properties of 2 Guna Collagen MDs: MD-Muscle and MD-Tissue.
– Authors – Operational sites
Nitecka-Buchta A., Walczynska-Dragon K., Batko-Kapustecka J.: Department of Temporomandibular Disorders, SMDZ Zabrze Unit – Medical University of Silesia, Katowice, Poland;
Wieckiewicz M.: Department of Experimental Dentistry, Faculty of Dentistry – Medical University of Wroclaw, Poland.
1) Foreword
Myofascial pain syndrome is a common disorder caused by trigger points, hard, localised, palpable nodules, that are painful on intermediate palpation. The anatomical damage is characterised by lesions of the myofilaments and sarcolemma. The functional damage is characterised by local hypoxia and the release of pro-inflammatory mediators (bradykinin, catecholamines, neuropeptides, cytokines) with persistent pain and inflammation. Certain close trigger points join to form areas of myogelosis, in which the level of O2 is extremely low, leading to a reduction in ATP.
– Lidocaine hydrochloride 2% is commonly used for local injection for nerve blocks and analgesia of the superficial tissues; the mechanism of action consists in blocking the Na+ channels of the cell membrane.
In trigger point therapy, it is used without a vasoconstrictor due to the risk of ischaemic necrosis. The duration of the analgesic effect varies from 30 minutes to 3 hours.
2) Purpose of the study
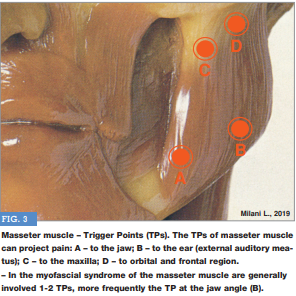
– Assessment of the efficacy of local intramuscular injections of Collagen Medical Device Muscle (MD-Muscle) or lidocaine in reducing the pain caused by trigger points in the masseter muscle (FIG. 3).
3) Materials and methods
3-1 Participants
From a group of 102 Caucasian patients treated at the Department of Temporomandibular Disorders – Medical University of Silesia, Katowice, Poland, 50 patients who had had chronic myofascial pain (MFP) of the masseter muscle for an average of 8.5 months were identified and included in the study.
3-2 Inclusion criteria
(1) Age ≥18 and ≤80 years; (2) Presence of myofascial pain in the masseter muscle according to Temporomandibular Disorder Diagnostic Criteria (DC/ TMD) (II.1.A. 2 and 3) (Peck et al., 2014); (3) Presence of latent or active trigger points in the masseter muscle(s) observed on palpation; (4) Patient consent to inclusion.
3-3 Exclusion criteria
(1) Patients undergoing dental treatment; (2) Patients on treatment with or dependence on analgesics and/or drugs affecting muscle function; (3) Patients who had had head or neck injuries in the previous 2 years; (4) Edentulous patients and those with occlusal contacts without arch supports; (5) Patients treated by a neurology specialist for neurological disorders and/or neuropathic pain and/or headache; (6) Patients who had had radiotherapy; (7) Odontogenic pain; (8) Pregnancy or breastfeeding; (9) Malignancies; (10) Severe mental disorders; (11) Drug and/or alcohol addiction; (12) Contraindications to injection therapy; (13) Patients with needle phobia; (14) Hypersensitivity to the substances involved in the study.

The 50 patients were split into 3 Groups using a simple computerised randomisation procedure: 1) Group I – MD-Muscle = 18; 2) Group II – lidocaine = 15; 3) Group III – sterile physiological solution = 17. After randomisation, 7 patients refused to take part in the study. The 3 Groups were therefore resized (43 patients) as follows (TAB. 2):
– Group I – Experimental group proper – Collagen MD-Muscle, 2 mL = 15 patients (5 M, 10 F), mean age 37.2 ± 4.97 years;
– Group II – Control group proper – lidocaine 2%, 2 mL = 13 patients (5 M, 8 F), mean age 42.8 ± 0.98 years;
– Group III – Neutral control group – sterile saline solution, 2 mL = 15 patients (7 M, 8 F), mean age 40.3 ± 1.18 years.
The 3 substances used in the trial were injected into the trigger point(s) identified [unilateral (40 patients), bilateral (3 patients)] by the same physician.
Patients were not told which substance would be injected. – Study design consisted in 4 steps: (1) screening for study participation and enrolment; (2) baseline - first injection; (3) 1st follow-up and second injection; (4) 2nd follow-up. The period elapsing between (2), (3) and (4) was one week (days 0, 7 and 14).
4) Measurement of treatment outcomes
– Visual-analogue scale (VAS 1-10) - days 0, 7 and 14. Primary outcome.
– Superficial electromyography (EMGs) - days 0, 7 and 14. Secondary outcome.
4-1 VAS
The average reduction in pain intensity at days 7 and 14 was (FIG. 4, TAB. 3):
– Group I – MD-Muscle = -4.3 (-53.75%). From 8 (baseline) to 4.6 (day 7) to 3.7 (day 14).
– Group II – lidocaine 2% = -2.3 (-25%). From 8.3 (baseline) to 7.4 (day 7) to 6 (day 14).
– Group III – sterile saline solution = -1.63 (-20.1%). From 8.13 (baseline) to 6.8 (day 7) to 6.5 (day 14).
.png)
.png)
Comments by the author
A) It can be observed that, unlike lidocaine, MD-Muscle was very efficacious even just 7 days after the first injection, with a 40% reduction in pain symptoms, which dropped further after the second injection.
B) The similarities in the results between lidocaine and sterile saline solution at both 7 and 14 days should come as no surprise, as lidocaine produces an analgesic effect that wears off within 3 hours from the injection. At day 14, the difference in VAS score was -2.3 for lidocaine and -1.63 for sterile saline solution.
C) Similarly, it should come as no surprise that sterile saline solution produces a modest analgesic effect when injected into a myofascial trigger point: the analgesic effect – in this case – is not due to the sterile saline solution in itself, rather to its mechanical effect and the stimulation of the Aδ and c nerve fibres that introducing a needle into a trigger point produces (Milani, 2003, 2004).
D) MD-Muscle is more than twice as efficacious as lidocaine 2% (-53.75% vs -25.0%).
4-2 EMGs
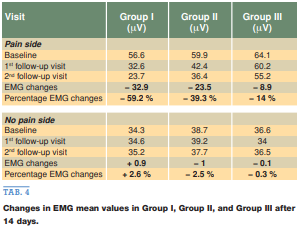
The mean reduction in the voltages recorded on days 7 and 14 was (FIG. 5, TAB. 4):
– Group I – MD-Muscle = -32.9 μV (-59.2%). From 56.6 μV (baseline) to 32.6 μV (day 7) to 23.7 μV (day 14).
– Group II – lidocaine 2% = -23.5 μV (-39.3%). From 59.9 μV (baseline) to 42.4 μV (day 7) to 36.4 μV (day 14).
– Group III – sterile saline solution = -8.9 μV (-14%). From 64.1 μV (baseline) to 60.2 μV (day 7) to 55.2 μV (day 14).
.png)
Comments by the author
A) The EMGs μV values given are the average values of 3 measurements.
B) The % differences for the EMGs values in Groups I and II are consistent with theVAS valuesfor the same Groups(see above).
C) In the study, the EMGs values for the same muscle on the asymptomatic side were also recorded in 40 patients [data shown in TAB. 4 (NP)].
5) Side effects
Approximately 30 minutes after the injection of MD-Muscle in the trigger point(s) identified in the masseter muscle(s), the patients reported an ache when opening their mouth, a slight local swelling feeling and mild local muscle stiffness. After about 1 hour, all these symptoms had disappeared.
In 9 patients out of 43 (21%), small bruises appeared at the needle introduction point(s) after the injection.
All these effects were temporary and completely reversible. No severe adverse effects occurred during the study.

