
+38(066)493-43-78
Показать все контакты
A NEW AND REFINED INJECTABLE TREATMENT FOR MUSCULOSKELETAL DISORDERS – BIOSCAFFOLD PROPERTIES OF COLLAGEN AND ITS CLINICAL USE
Leonello Milani, MD, PhD
– Vice President the International Academy of Physiological Regulatoring Medicine
– Vice President A.I.O.T.
– Scientific Director La Medicina Biologica and of Physiological Regulating Medicine
Via Palmanova, 1
I – 20132 Milano
SUMMARY
Connective tissue and collagen in particular – a real protein-tissue – progressively degrade and reveal to be inadequate to perform the functions they are to accomplish in each organism. This is due to aging, sedentarity, intense physical activity or inadequate sports activity, postural alteration, alimentary disequilibrium, and PNEI-axis alteration. Specific injectable Medical Devices (MD) (both distrectual and tissular) represent a new and refined tool in prevention and therapy to treat the ageing of articular structures, as well as periarticular ones and those concerning mesodermic supporting tissues. These MDs replace the lack of collagen, which is always recurrent in the inflammatory and/or degenerative diseases of the locomotor Apparatus and other anatomical structures of mesodermic origin; they are natural, free from negative side effects (excellent safety); they can be associated with homotoxicological therapies as well as allopathic ones that are being applied or that will be scheduled; moreover, they can be associated with physical therapies. Non-invasiveness of injections using Guna MDs – which are the first to highlight quality therapeutic results in 7 controlled clinical trials [Registration Dossier c/o Istituto Superiore di Sanità (Italian Superior Health Institute)] – together with other characteristics such as effectiveness, tolerability, absence of allergic reactions and their natural origin make them a valuable tool in standard procedures (both in treatments by specialists or general practictioners) and in processes aimed at improving the patients’ quality of life, which could otherwise worsen or become further chronic
KEY WORDS: COLLAGEN, MEDICAL DEVICE, ANCILLARY SUBSTANCE, GUNA MEDICAL DEVICE, PAIN, OSTEO-ARTHRO-MYO-FASCIAL PATHOLOGIES.
COLLAGEN – COMPOSITION AND ACTION
Collagen is the most abundant protein (structural protein – tissue; molecular weight 300KDa) in mammalians’ organism – accounting for about 5-6% of an adult’s body weight (Van der Rest et Al., 1991); one third (Trentham et Al., 1977) or one fourth (Lynsenmeyer, 1991) of the whole protein mass of higher animals is composed of collagen: bones and tendons, joint capsules and muscles, ligaments and fascia, teeth and serous membranes, the skin and the extracellular matrix (ECM).
– According to some hypotheses, the ancestral gene that synthesizes collagen has evolved to its present form due to further mutations starting from one single unit composed of only 54 base pairs of DNA.
At present the alpha 2 collagen gene is composed of about 38.000 base pairs.
– The basic difference between functional proteins, which are involved in biochemical, enzymatic, immune, membrane and/or transmembrane receptor processes, and structural proteins, which play an important role in building the scaffold of higher organisms (connective tissue in a wider sense and more specifically – fibrous tissue) is not considered so important for collagen.
For example, collagen VI plays an essential role in the processes of cell adhesion, replication and survival through its interaction (cross-talk) with integrins and/or other transmembrane receptors (Pfaff et Al., 1993; Jan et Al., 2004), showing both roles: the genetic absence of Collagen VI causes severe morpho-functional alterations of muscle fibres and apoptosis by acting directly on the mitochondrion (Rizzuto, 2003) due to a failure to regulate cell permeability (last author mentioned).
– Collagen “health” is ultimately the individual’s health: man’s peak of collagen biosynthesis occurs between 45 and 60 years of age (Heine, 2009): after that age there is a rapid decrease of collagen that is also accompanied by a rapid decrease of elastin and proteoglycans (Milani, 2004 a) (FIG. 1).
.png)
An insufficient renewal of the ECM brings about a sluggish function of the Transit System (Pischinger, 1983). Faulty routing of waste will cause the accumulation of toxins usually directed by the cells in the microvessels of the lymphatic system; this impacts oxygenation of tissues, nutrient assimilation and hydration. Fragility and sclerosis are silent symptoms preceding degeneration and possible tissue dedifferentiation (disease evolution according to Reckeweg).
.png) The base unit of collagen is tropocollagen (FIG. 2), a glycoprotein composed of three left-handed helices of polypeptide units carrying glucose and galactose molecules that are attached only to the molecule of the amino acid hydroxylysine (Hyl), one of the only four amino acids that form tropocollagen with Glycine (Gly), Proline (Pro) and 4-Hydroxyproline (Hyp).
The base unit of collagen is tropocollagen (FIG. 2), a glycoprotein composed of three left-handed helices of polypeptide units carrying glucose and galactose molecules that are attached only to the molecule of the amino acid hydroxylysine (Hyl), one of the only four amino acids that form tropocollagen with Glycine (Gly), Proline (Pro) and 4-Hydroxyproline (Hyp).
Tropocollagen has some interesting structural “anomalies” compared to other proteins:
– In the molecule:
1) Every triplet of amino acids always starts with Glycine (Gly-A-B);
2) The amino acid sequence is often represented by the triplet Gly-ProHyp;
3) These triplets cannot usually be found in other proteins and have to be considered unique and special;
4) Proline determines the twisting, the “change of direction” along the axis of the protein strand; that’s why it is absolutely absent in globular proteins;
5) Many residues of Hyp have two sugar residues. Therefore, collagen is a glycoprotein (great amount of protein – small amount of sugar) and not a proteoglycan (PG) (great amount of sugar – small amount of protein); The collagen imbalance of sugar/protein ratio balances that of PGs.
6) Axial periodicity (text, see after: FIG. 6), a true metamerism that is visible only with the electron microscope.
These “anomalies” guarantee a perfect strength and function of the molecule: when the three polypeptide units are intertwined in a tight triple helix, stabilized between hydroxylated amino acids (crosslinks) by weak H+ bonds, they give basic and special characteristics to collagen 2: structural strength and organoleptic rigidity. The spatial configuration of tropocollagen is a cylindrical braid composed of three rods wrapped in an helix. This gives the molecule great resistance and flexibility: to break a 1 mm diameter collagen fiber an 11 kg weight must be applied to each end.
The hydrogen bond is a weak, noncovalent bond: it is the number of atoms that gives it its strength, as it occurs with fibroin, the structural protein of silk.
The hydroxylation of Pro and Hyp and the hydroxylation of Lys and Hyl occur thanks to the cofactor ascorbic acid (Vitamin C) and to the substrate acidum α-ketoglutaricum, one of the three-carboxylic acids of Krebs’ Cycle. A deficit of one of these metabolic boosters will cause severe alterations of the connective tissue which can manifest as scurvy and cancer cachexia.
A failed hydroxylation to Hyp and Hyl leads to the formation of a collagen fibril that is structurally and functionally impaired.
According to the different types of collagen involved some severe genetic cases of Osteogenesis imperfecta, Bethlem myopathy, Ulrich’s scleroatonic muscular dystrophy, mitochondrial myopathy may occur, just to mention a few that illustrate the truth behind Garrod’s “old” theory (1902) – “one gene, one enzyme” which still applies today.
► The diseases due to an acquired collagen deficiency are also thought to have their pathogenesis in a faulty synthesis and use of collagen (TAB. 1).
– I would like to remind that Lys, precursor of tropocollagen 5-Hyl is an essential amino acid that must be sourced from food and/or from supplementation.
– Collagen biosynthesis is carried out by different cell lines (fibroblasts in the loose and fibrous fibrillar connective tissue, osteoblasts in bones, chondroblasts in cartilage, etc.)
After the amino acids interlock, the globular procollagen is produced at an intracellular level and is pushed outwards through the Golgi apparatus (Olsen, 1983) (FIG. 3). Here, thanks to the shortening of the 2 telomeres (one N-terminal, the other C-terminal), the procollagen turns into protocollagen; as soon as protocollagen is being formed, this produces a negative feedback on the collagenous-genetic cell, by inhibiting a further synthesis.
– The procollagen microfibrils are therefore polymerized outside the collagenous-genetic cell.
The single units of protocollagen are staggered thanks to Lysyl-oxidase, linearly and in parallel array to gradually form one microfibril, one subfibril, and one collagen fibril. (FIG. 4).
Several collagen fibrils constitute a collagen fibre.
.png)
.png)
–This process is thought to occur, at least partly, via an autocatalytic route (Prockop, 2004; Cisneros et Al., 2006).
In some rare moments biology by-passes the rigid genetic determinism and the most flexible epigenetic possibilism and shows great adaptability supported by autocatalysis with more flexibility and adaptability (Lima de Faria, 2003).
This undermines deeply the Darwinian and post-Darwinian pure evolutionary theory (Milani, 2009).
.png)
– The fibrils are characterized by a periodicity: they show small structural units along their own course which repeat every 670 Amstrong [FIGG. 5 (1, 2), 6].
.png)
– The reason for this periodicity (a true structural form), which has been sought for a long time, is simple: as both fibrils and the collagen fibres are much longer than the maximum diameter of the cells that synthesize them, the basic collagen molecules must be small enough to be secreted and polymerized afterwards.
.png)
If a tropocollagen fibre is 2,800 Amstrong long, how can we justify a 670 Amstrong axial periodicity? This is possible only if the underlying fibrils are out of phase of one quarter compared to the overlapping fibrils (Hodge and Petruska model, 1964) and if these do not relate by the ends but rather line up in a way that there is a half length period between their own extremities (1 dark segment + 1 light segment = 1 period).
Each molecule of tropocollagen is composed of 5 light segments spaced out by 4 dark segments. Thanks to the use of Conventional Amplitude Modulation (AC Imaging) structural models have been recently proposed, different from the traditional model that is recognized by the scientific community (Bozel et Al., 2007), even if a new convincing molecular scheme has not yet been defined (Jiang et Al., 2009).
► Such arrangement of the fibrils in the formation of collagen fibres guarantees a great strength in terms of:
– RESISTANCE, NON-EXTENSIBILITY, NON-COMPRESSIBILITY, but also PLASTICITY FLEXIBILITY, LOAD RESISTANCE , TORSION RESISTANCE
These characteristics make collagen an extremely versatile “structure” that Nature has been selecting during hundreds of millions of years and upheld as the best means to fulfil its many functions.
GUNA MEDICAL DEVICES FOR THE INJECTIVE TREATMENT OF DYSFUNCTIONAL AND PAINFUL ARTHRO MYOFASCIAL PATHOLOGIES
A new substantial and refined approach to the painful dysfunctional pathologies of the musculoskeletal system and of the related motor functions is now offered by Guna Medical Devices for use in clinical practice and in specialist facilities.
The 13 Guna Medical Devices (MD) contain collagen and ancillary substances of natural origin (TAB. 2).
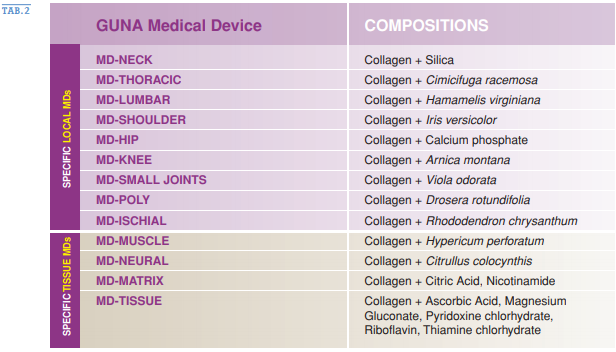
The ancillary substances allow a more effective and specific placement of collagen and have the function of conveying and stabilization.
►Eight of these MD are specific of the individual anatomical skeletal areas and of the disorders connected with them: MD-NECK, MD-THORACIC, MDLUMBAR, MD-SHOULDER, MD-HIP, MD-KNEE, MD-SMALL JOINTS, MDPOLY (multi-articular)]; one is specific for the sciatic nerve [MD-ISCHIAL], and four others that are specific for tissue diseases, derived predominantly from mesodermal tissue: MD-MUSCLE, MD-NEURAL, MD-MATRIX (Extra Cellular Matrix), MD-TISSUE (soft tissues) (TAB. 2; FIG. 12).
.png) All 13 Guna MD contain, in addition to the carrier excipient (ancillary), collagen of porcine origin.
All 13 Guna MD contain, in addition to the carrier excipient (ancillary), collagen of porcine origin.
–The swine tissues have a very high average content of collagen (22.8% Glycine, Proline = 13.8%; HydroxyProline = 13%).
The average content of the other amino acids is only 3% (max Glutamic acid = 9.5%; min Tyrosine = 0.4%): the 50% is then made up of collagen.
Thanks to the particular process of tangential filtration, sterilization and control of molecular weight, a pure product (without contaminants) is obtained, that has the standard chemical and physical characteristics of a good and clinical safety.
The purpose of the local administration of this biomaterial “where it is needed” is structural: to replace, strengthen, structure and protect (adhesion barrier) the cartilage, the tendons, the ligaments, the joint capsules, etc.; to improve the structure of collagen fibers and - consequently - of all anatomical structures in which it is present; to provide mechanical support to the district concerned.
– One of the most important causes of district joint pain is the laxity of the intra-and extra-articular stabilization structures; the loose restraint systems determine joint hypermobility, especially in not physiological directions and angles that wear and tear early the restraint systems themselves and act towards a progressive degeneration of the cartilage.
The infiltration of collagen and the single ancillary ingredients, is perfectly tolerated by the patient and devoid of adverse reactions. It is physiological, compatible and does not cause microinflammation with subsequent fibrotic retraction, as in prolotherapy, which covers basically the same purpose: the stabilization of periartricular structures.

